Medical Records ROI Crystal Clinic Orthopaedic Center. A general authorization for the release of medical or other information is not sufficient for this purpose.
Https My Clevelandclinic Org Scassets Files Org Online Services Mychart Pediatric Proxy Form Ashx La En
41112 AUTHORIZATION FOR THE RELEASE OF MEDICAL INFORMATION FROM MAIN CAMPUS OF THE CLEVELAND CLINIC Health Data Services Ab-7 9500 Euclid Avenue.
Cleveland clinic medical release form. Fill out the requested boxes that are yellow-colored. Release of Information Form Spanish Important Steps. Whenever your request for access to your health information is denied by Cleveland Clinic Akron General in whole or part you.
Authorizations must be signed and dated in order to be processed. Check and initial the appropriate boxes. Complete all fields on the authorization form s when requesting the release of your records.
Enter the path to this folder in the folder provider. Your medical records are confidential documents protected by privacy laws. Once opened right click on the file to print or save a copy of the PDF to your computer.
7722875200 200 SE Hospital Ave. Open the form in the feature-rich online editor by hitting Get form. Please indicate if you have a pending doctors appointment at the time of request to expedite this release.
Cleveland Clinic Martin Health. Checking the box below and returning this form to the Director of. Our award-winning Emergency Department operates 24 hours a day 7 days a week.
If you do not know your Cleveland Clinic number leave it blank. Authorization for the release of medical information th. The path must be relative to the root of the.
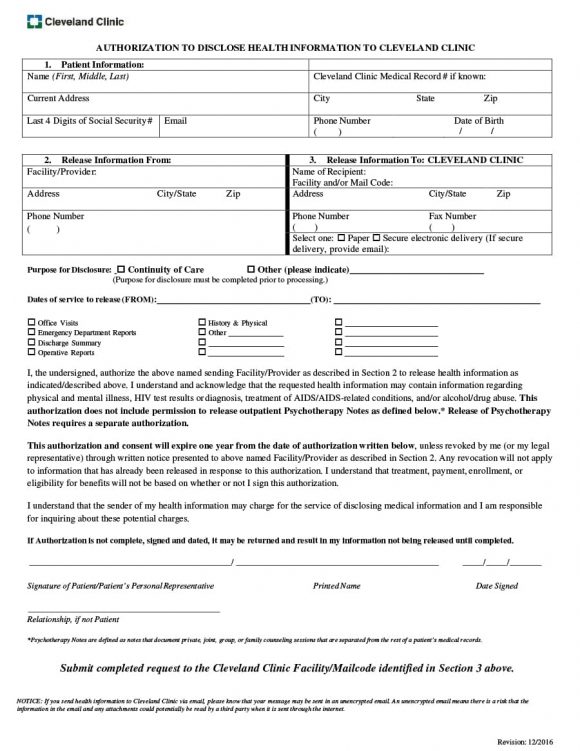
This form is to be used by a patient or legal representative to authorize the release of information to a third party other than a family member or friend such as an insurance company employer or for legal purposes etc. AUTHORIZATION TO DISCLOSE HEALTH INFORMATION TO CLEVELAND CLINIC 1. Health Information Management Attn.
Patient Information Name First Middle Last Cleveland Clinic Medical Record if known. After the form s is signed and dated fax the information to the number indicated at the top of the form or mail it to the address indicated. Complete the authorization Click here to download the form.
Health Visit Form Employee Health Plan Wellness Program. Include a copy of your photo identification with signature. Patient Name First Middle and Last Cleveland Clinic Medical Record Current Address Mailing address if different from current address City State Zip.
Box 9010 Stuart FL 34995 View All Locations. Please print and complete the appropriate form below or call us and we will fax the form to you. Patient requests are generally processed by our copy service within 10 business days.
Click on the buttons below to open a fillable-PDF. The federal rules restrict any use of. Pharmacy Management Prior Authorization Form Caremark Out of Pocket Prescription Reimbursement Form Cleveland Clinic EHP Appeal Form EHP Medical Management Request for Prior Authorization Form.
Select the folder type. If you do not know your Cleveland Clinic medical record number leave it blank. Cleveland Clinic Abu Dhabi Al Maryah Island Abu Dhabi.
Each section needs to be completed to be valid. 800 CCAD 3 800 222 33 From outside the UAE 971 2 659 0200. The path entered is relative to the root of the provider so if the field is left empty then the folder will map to the provider root.
After the form is completed signed and dated. The following tips will allow you to complete FL Cleveland Clinic Authorization for the Release of Medical Information Through Drconnect easily and quickly. Current Address City State Zip Last 4 Digits of Social Security Email Phone Number Date of Birth 2Release Information From.
Please send this form to. To request a copy of your medical records. EHR RK2-1 6801 Brecksville Rd Independence OH 44131 SECTION A Patient information.
Complete all fields on the authorization forms when requesting the release of your records. Fill out all the information that applies to your request. Alternatively you can complete our online form and receive a callback to confirm your appointment.
To get a copy of your medical records from your hospital stay lab tests or diagnostic imaging you must fill out and sign a release form see links below. Requisitions Forms Test requisitions pathology documentation pathology consultation kit instructions and patient billing forms are available to download here. The authorization form must be signed and dated.
Release of Information Form.
Https My Clevelandclinic Org Scassets Files Org Functional Medicine Release Of Information From Other Facilities Ashx La En
 Cleveland Clinic Authorization Release Form 2020 2021 Fill And Sign Printable Template Online Us Legal Forms
Cleveland Clinic Authorization Release Form 2020 2021 Fill And Sign Printable Template Online Us Legal Forms
 Cleveland Clinic Discharge Signnows Fill Out And Sign Printable Pdf Template Signnow
Cleveland Clinic Discharge Signnows Fill Out And Sign Printable Pdf Template Signnow
 Cleveland Clinic Medical Records Fax Number Fill Online Printable Fillable Blank Pdffiller
Cleveland Clinic Medical Records Fax Number Fill Online Printable Fillable Blank Pdffiller
Https Ewebapps Ccf Org Myimages Content Help Myimagesreleaseauthorization Pdf
 Cleveland Clinic Medical Release Form Fill Out And Sign Printable Pdf Template Signnow
Cleveland Clinic Medical Release Form Fill Out And Sign Printable Pdf Template Signnow
Https Drconnect Clevelandclinic Org Files Drconnectnhimplementationoverview Pdf
 Cleveland Clinic Medical Records Fax Number Fill Online Printable Fillable Blank Pdffiller
Cleveland Clinic Medical Records Fax Number Fill Online Printable Fillable Blank Pdffiller
 Cleveland Clinic Authorization Release Form Fill Online Printable Fillable Blank Pdffiller
Cleveland Clinic Authorization Release Form Fill Online Printable Fillable Blank Pdffiller
Https My Clevelandclinic Org Scassets Files Org Patients Visitors Information Records Release Other Facilities Ashx La En
Https Drconnect Clevelandclinic Org Files Drconnectphysicianimplementationoverview Pdf
 40 Medical Records Release Form Release Of Information
40 Medical Records Release Form Release Of Information
Https My Clevelandclinic Org Ccf Media Files Patients Records Release Form Pdf
Cleveland Clinic Medical Records Fax Number Fill Online Printable Fillable Blank Pdffiller
Comments
Post a Comment